In my practice, I often see hip fractures as one of the most urgent orthopaedic problems affecting older adults, though younger patients can also suffer them after road traffic accidents, falls from height, or other major trauma. A hip fracture is not just a broken bone. It is often a life-changing event because it can suddenly take away mobility, independence, confidence, and even the ability to manage basic daily tasks without support.[1]
For Bangladeshi patients and families, the first few hours after a hip fracture are usually filled with confusion. Many people ask whether the bone can heal on its own, whether surgery is always required, and how quickly the operation needs to happen. I usually explain that most true hip fractures do need surgical treatment, and early movement after surgery is one of the main reasons we operate.[1][2]
What a hip fracture actually means
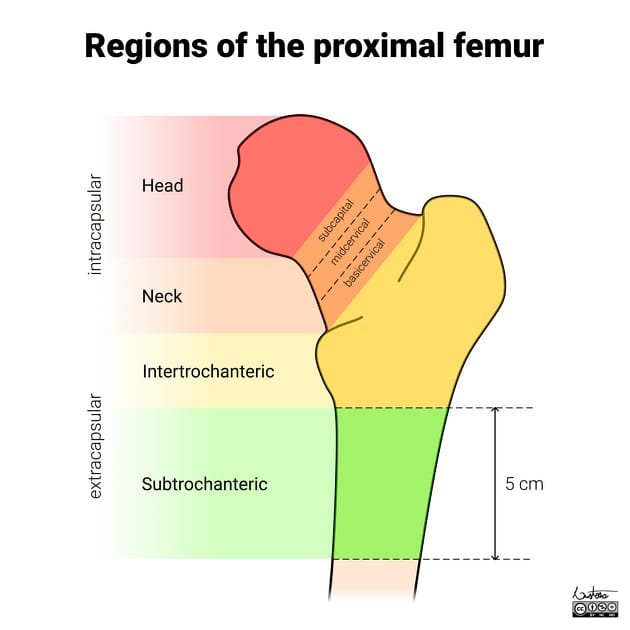
A hip fracture is a break in the upper part of the femur, or thigh bone, close to the hip joint. The most common locations are the femoral neck and the intertrochanteric region, while subtrochanteric fractures occur a little lower down. The exact location matters because it affects which operation is most appropriate and what the recovery may look like.[1]
In older adults, the usual cause is a low-energy fall, often inside the home. In younger people, hip fractures are more likely to happen after high-energy injuries such as a motorcycle crash or a major fall. In Bangladesh, both patterns are common. I see elderly patients who slipped in the bathroom or courtyard, and I also see younger trauma patients injured on busy roads.[1]
Why hip fractures are treated urgently
Hip fractures are very painful and usually make standing or walking impossible. Beyond pain, the real danger is what happens if a patient stays in bed too long. Prolonged immobility increases the risk of bed sores, blood clots, pneumonia, deconditioning, and confusion in older adults.[1]
This is why prompt surgery is usually recommended. AAOS notes that most hip fractures require surgery, and operating as soon as possible, often within 24 to 48 hours, may reduce complications.[1] NICE also recommends surgery on the day of, or the day after, admission whenever possible, while correcting urgent medical issues that could make surgery unsafe.[2]
One important point I want Bangladeshi families to understand is that “quick surgery” does not mean “rushed surgery.” The patient still needs proper medical optimization. If someone has uncontrolled diabetes, severe anemia, dehydration, anticoagulation problems, or an acute chest infection, these must be addressed without creating avoidable delay.[2]
Common signs of a hip fracture
The typical symptoms are quite striking. Patients often describe:
- sudden severe pain in the groin or upper thigh
- inability to stand or bear weight
- pain when trying to move the leg
- a shorter-looking leg on the injured side
- outward rotation of the leg
- swelling or bruising around the hip or thigh
Some nondisplaced fractures can be more subtle, and a patient may still move the leg a little or even try to stand, though it is usually very painful.[1] That is why an elderly person with hip pain after a fall should not be ignored just because they are still able to move.
How I evaluate a patient before recommending surgery
When I evaluate patients with this problem, I first confirm whether it is truly a hip fracture and whether there are other injuries or medical issues that change the treatment plan.
History and examination
I want to know how the injury happened, the patient’s age, their usual walking ability, what diseases they already have, whether they use blood thinners, and whether they were independent before the injury. In Bangladesh, this part is important because surgery planning should fit the person’s real functional goals and home support situation.
Imaging
X-rays are the main first test and diagnose most hip fractures.[1] If the X-ray does not show a fracture clearly but suspicion remains high, more imaging may be needed. NICE recommends MRI when hip fracture is suspected despite negative X-rays, or CT if MRI is not available within 24 hours or cannot be done.[2]
Medical optimization
Before surgery, patients often need blood tests, cardiac review, and anesthesia assessment. If there is dehydration, anemia, uncontrolled sugar, or a chest infection, these problems must be corrected promptly.[1][2]
The main types of hip fracture surgery
Hip fracture surgery is not one single operation. The procedure depends on the fracture location, whether the bone fragments are displaced, the patient’s age, bone quality, and functional goals.
1. Fixation for nondisplaced femoral neck fracture
If the femoral neck fracture is not displaced, internal fixation may be used. This usually means pins, screws, or a plate-and-screw device to hold the fracture in position while it heals.[1]
In carefully selected younger or healthier patients, preserving the natural femoral head is often the priority. That is because replacing the hip is not always the best first choice for every patient with a fracture.
2. Hemiarthroplasty or total hip replacement for displaced femoral neck fracture
Displaced fractures of the femoral neck are more difficult because the blood supply to the femoral head may be damaged. This raises the risk of nonunion and avascular necrosis.[1]
For many older patients, hemiarthroplasty, which is a partial hip replacement, is commonly chosen.[1] In selected patients, total hip replacement may also be considered, especially when activity level, joint condition, and overall health support that choice.[1]
I usually explain to families that the aim is not only to fix the X-ray. The aim is to choose the method that gives the patient the best chance to sit, stand, transfer, and walk again safely.
3. Intertrochanteric fracture fixation
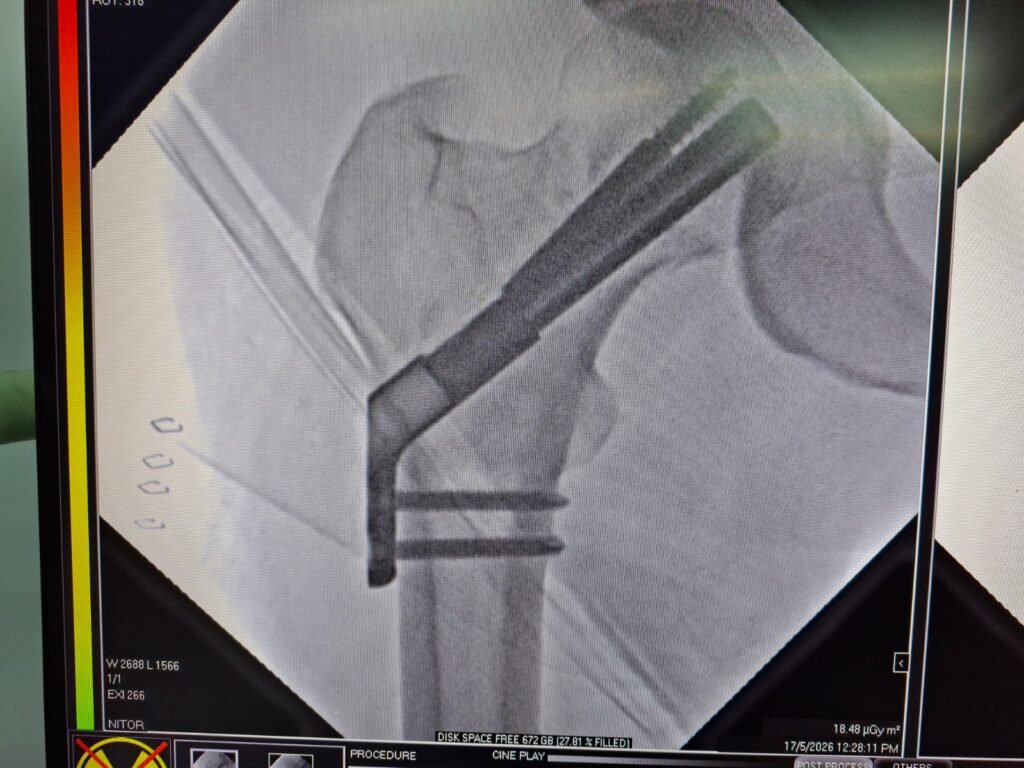
Intertrochanteric fractures are usually treated with either a sliding compression hip screw and side plate or an intramedullary nail.[1] The choice depends on the fracture pattern and stability.
These operations are designed to hold the fracture while still allowing useful movement and rehabilitation. In many cases, getting the fixation right is what makes early mobilization possible.
4. Subtrochanteric fracture fixation
Subtrochanteric fractures often need intramedullary nailing, sometimes with additional locking screws or plating strategies depending on the fracture configuration.[1] These injuries may be seen after significant trauma, though they can also occur in fragile bone.